Cardiac arrest

Cardiac arrest
| Cardiac arrest | |
|---|---|
| Other names | Cardiopulmonary arrest, circulatory arrest, sudden cardiac arrest (SCA), sudden cardiac death (SCD)[1] |
| CPRbeing administered during a simulation of cardiac arrest. | |
| Specialty | Cardiology,emergency medicine |
| Symptoms | Loss of consciousness,abnormal or no breathing[1][2] |
| Usual onset | Older age[3] |
| Causes | Coronary artery disease,congenital heart defect, majorblood loss, lack of oxygen,very low potassium,heart failure[4] |
| Diagnostic method | Finding no pulse[1] |
| Prevention | Not smoking, physical activity, maintaining a healthy weight[5] |
| Treatment | Cardiopulmonary resuscitation(CPR),defibrillation[6] |
| Prognosis | Survival rate ~ 10% (outside of hospital) 25% (in hospital)[7][8] |
| Frequency | 13 per 10,000 people per year (outside hospital in the US)[9] |
Cardiac arrest is a sudden loss of blood flow resulting from the failure of the heart to effectively pump.[10] Signs include loss of consciousness and abnormal or absent breathing.[1][2] Some individuals may experience chest pain, shortness of breath, or nausea before cardiac arrest.[2] If not treated within minutes, it typically leads to death.[10]
The most common cause of cardiac arrest is coronary artery disease.[4] Less common causes include major blood loss, lack of oxygen, very low potassium, heart failure, and intense physical exercise.[4] A number of inherited disorders may also increase the risk including long QT syndrome.[4] The initial heart rhythm is most often ventricular fibrillation.[4] The diagnosis is confirmed by finding no pulse.[1] While a cardiac arrest may be caused by heart attack or heart failure, these are not the same.[10]
Prevention includes not smoking, physical activity, and maintaining a healthy weight.[5] Treatment for cardiac arrest includes immediate cardiopulmonary resuscitation (CPR) and, if a shockable rhythm is present, defibrillation.[6] Among those who survive, targeted temperature management may improve outcomes.[11][12] An implantable cardiac defibrillator may be placed to reduce the chance of death from recurrence.[5]
In the United States, cardiac arrest outside hospital occurs in about 13 per 10,000 people per year (326,000 cases).[9] In hospital cardiac arrest occurs in an additional 209,000.[9] Cardiac arrest becomes more common with age.[3] It affects males more often than females.[3] The percentage of people who survive with treatment is about 8%.[7] Many who survive have significant disability.[7] However, many American television programs have portrayed unrealistically high survival rates of 67%.[7]
| Cardiac arrest | |
|---|---|
| Other names | Cardiopulmonary arrest, circulatory arrest, sudden cardiac arrest (SCA), sudden cardiac death (SCD)[1] |
| CPRbeing administered during a simulation of cardiac arrest. | |
| Specialty | Cardiology,emergency medicine |
| Symptoms | Loss of consciousness,abnormal or no breathing[1][2] |
| Usual onset | Older age[3] |
| Causes | Coronary artery disease,congenital heart defect, majorblood loss, lack of oxygen,very low potassium,heart failure[4] |
| Diagnostic method | Finding no pulse[1] |
| Prevention | Not smoking, physical activity, maintaining a healthy weight[5] |
| Treatment | Cardiopulmonary resuscitation(CPR),defibrillation[6] |
| Prognosis | Survival rate ~ 10% (outside of hospital) 25% (in hospital)[7][8] |
| Frequency | 13 per 10,000 people per year (outside hospital in the US)[9] |
Signs and symptoms
Cardiac arrest is preceded by no warning symptoms in approximately 50 percent of people.[13] For those who do experience symptoms, they will be non-specific, such as new or worsening chest pain, fatigue, blackouts, dizziness, shortness of breath, weakness and vomiting.[14] When cardiac arrest occurs, the most obvious sign of its occurrence will be the lack of a palpable pulse in the victim. Also, as a result of loss of cerebral perfusion (blood flow to the brain), the victim will rapidly lose consciousness and will stop breathing. The main criterion for diagnosing a cardiac arrest, as opposed to respiratory arrest, which shares many of the same features, is lack of circulation; however, there are a number of ways of determining this. Near-death experiences are reported by 10 to 20 percent of people who survived cardiac arrest.[15]
Causes
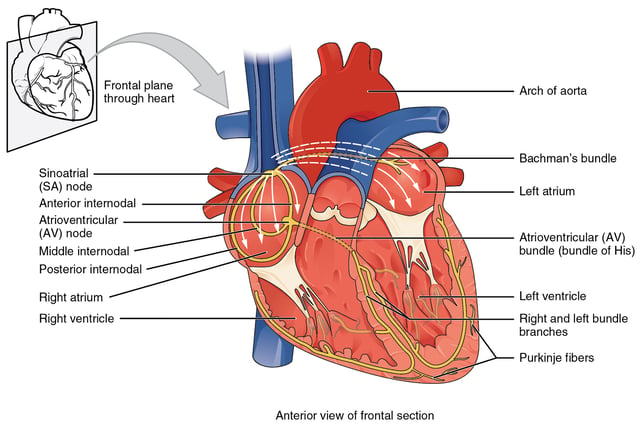
Conduction system of heart
Sudden cardiac arrest (SCA) and sudden cardiac death (SCD) occur when the heart abruptly begins to beat in an abnormal or irregular rhythm (arrhythmia). Without organized electrical activity in the heart muscle, there is no consistent contraction of the ventricles, which results in the heart's inability to generate an adequate cardiac output (forward pumping of blood from heart to rest of the body).[18] There are many different types of arrhythmias, but the ones most frequently recorded in SCA and SCD are ventricular tachycardia (VT) or ventricular fibrillation (VF).[19]
Sudden cardiac arrest can result from cardiac and non-cardiac causes including the following:
Coronary artery disease
Cases have shown that the most common finding at postmortem examination of sudden cardiac death (SCD) is chronic high-grade stenosis of at least one segment of a major coronary artery,[22] the arteries that supply the heart muscle with its blood supply.
Structural heart disease
Structural heart disease not related to CAD (i.e. hypertrophic cardiomyopathy, congenital coronary artery anomalies, myocarditis) account for 10% of all SCDs.[18][21] Examples of these include: cardiomyopathy, cardiac rhythm disturbances, myocarditis, hypertensive heart disease,[21] and congestive heart failure.[24]
Left ventricular hypertrophy is thought to be a leading cause of SCD in the adult population.[25] This is most commonly the result of longstanding high blood pressure which has caused secondary damage to the wall of the main pumping chamber of the heart, the left ventricle.[26]
Congestive heart failure increases the risk of SCD fivefold.[24]
Inherited arrhythmia syndromes
Arrhythmias that are not due to structural heart disease account for 5 to 10% of sudden cardiac arrests.[27][28][29] These are frequently caused by genetic disorders that lead to abnormal heart rhythms. The genetic mutations often affect specialised proteins known as ion channels that conduct electrically charged particles across the cell membrane, and this group of conditions are therefore often referred to as channelopathies. Examples of these inherited arrhythmia syndromes include Long QT syndrome, Brugada Syndrome, Catecholaminergic polymorphic ventricular tachycardia, and Short QT syndrome. Other conditions that promote arrhythmias but are not caused by genetic mutations include Wolff-Parkinson-White syndrome.[18]
Long QT syndrome, a condition often mentioned in young people's deaths, occurs in one of every 5000 to 7000 newborns and is estimated to be responsible for 3000 deaths each year compared to the approximately 300,000[30] cardiac arrests seen by emergency services.
These conditions are a fraction of the overall deaths related to cardiac arrest, but represent conditions which may be detected prior to arrest and may be treatable.
Non-cardiac causes
The most common non-cardiac causes are trauma, bleeding (such as gastrointestinal bleeding, aortic rupture, or intracranial hemorrhage), overdose, drowning and pulmonary embolism.[31] Cardiac arrest can also be caused by poisoning (for example, by the stings of certain jellyfish).
Mnemonic for reversible causes
- Hs
- Ts
TabletsToxins
Cardiac Tamponade
Tension pneumothorax – A collapsed lung
Thrombosis (Myocardial infarction) – Heart attack
Thromboembolism (Pulmonary embolism) – A blood clot in the lung
Traumatic cardiac arrest
Risk factors
The risk factors for SCD are similar to those of coronary artery disease and include age, cigarette smoking, high blood pressure, high cholesterol, lack of physical exercise, obesity, diabetes, and family history.[34] A prior episode of sudden cardiac arrest also increases the risk of future episodes.[35]
Air pollution is also associated with the risk of cardiac arrest.[36] Current cigarette smokers with coronary artery disease were found to have a two to threefold increase in the risk of sudden death between ages 30 and 59. Furthermore, it was found that former smokers’ risk was closer to that of those who had never smoked.[13][37]
Mechanism
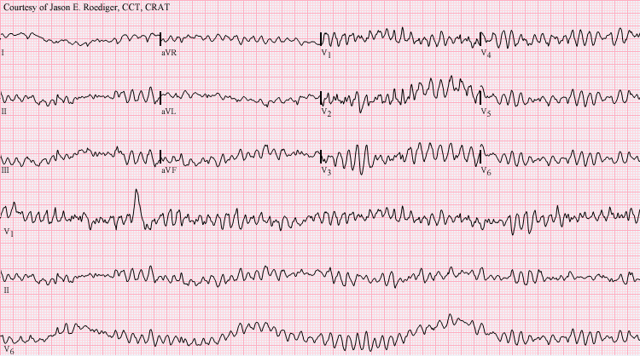
Ventricular fibrillation
The mechanism responsible for the majority of sudden cardiac deaths is ventricular fibrillation.[4] Structural changes in the diseased heart as a result of inherited factors (mutations in ion-channel coding genes for example) cannot explain the suddenness of SCD.[38] Also, sudden cardiac death could be the consequence of electric-mechanical disjunction and bradyarrhythmias.[39][40]
Diagnosis
Cardiac arrest is synonymous with clinical death. A cardiac arrest is usually diagnosed clinically by the absence of a pulse. In many cases lack of carotid pulse is the gold standard for diagnosing cardiac arrest, as lack of a pulse (particularly in the peripheral pulses) may result from other conditions (e.g. shock), or simply an error on the part of the rescuer. Nonetheless, studies have shown that rescuers often make a mistake when checking the carotid pulse in an emergency, whether they are healthcare professionals[41] or lay persons.[42]
Owing to the inaccuracy in this method of diagnosis, some bodies such as the European Resuscitation Council (ERC) have de-emphasised its importance.
The Resuscitation Council (UK), in line with the ERC's recommendations and those of the American Heart Association,[33] have suggested that the technique should be used only by healthcare professionals with specific training and expertise, and even then that it should be viewed in conjunction with other indicators such as agonal respiration.[32]
Various other methods for detecting circulation have been proposed.
Guidelines following the 2000 International Liaison Committee on Resuscitation (ILCOR) recommendations were for rescuers to look for "signs of circulation", but not specifically the pulse.[33] These signs included coughing, gasping, colour, twitching and movement.[45] However, in face of evidence that these guidelines were ineffective, the current recommendation of ILCOR is that cardiac arrest should be diagnosed in all casualties who are unconscious and not breathing normally.[33] Another method is to use molecular autopsy or postmortem molecular testing which uses a set of molecular techniques to find the ion channels that are cardiac defective.
Classifications
Clinicians classify cardiac arrest into "shockable" versus "non–shockable", as determined by the ECG rhythm. This refers to whether a particular class of cardiac dysrhythmia is treatable using defibrillation.[32] The two "shockable" rhythms are ventricular fibrillation and pulseless ventricular tachycardia while the two "non–shockable" rhythms are asystole and pulseless electrical activity.[46]
Prevention
With positive outcomes following cardiac arrest unlikely, an effort has been spent in finding effective strategies to prevent cardiac arrest.
With the prime causes of cardiac arrest being ischemic heart disease, efforts to promote a healthy diet, exercise, and smoking cessation are important. For people at risk of heart disease, measures such as blood pressure control, cholesterol lowering, and other medico-therapeutic interventions are used. A Cochrane review published in 2016 found moderate-quality evidence to show that blood pressure-lowering drugs do not appear to reduce sudden cardiac death.[47]
Code teams
In medical parlance, cardiac arrest is referred to as a "code" or a "crash".
This typically refers to "code blue" on the hospital emergency codes. A dramatic drop in vital sign measurements is referred to as "coding" or "crashing", though coding is usually used when it results in cardiac arrest, while crashing might not. Treatment for cardiac arrest is sometimes referred to as "calling a code".
People in general wards often deteriorate for several hours or even days before a cardiac arrest occurs.[32][48] This has been attributed to a lack of knowledge and skill amongst ward-based staff, in particular a failure to carry out measurement of the respiratory rate, which is often the major predictor of a deterioration[32] and can often change up to 48 hours prior to a cardiac arrest. In response to this, many hospitals now have increased training for ward-based staff. A number of "early warning" systems also exist which aim to quantify the person's risk of deterioration based on their vital signs and thus provide a guide to staff. In addition, specialist staff are being used more effectively in order to augment the work already being done at ward level. These include:
Crash teams (or code teams) – These are designated staff members with particular expertise in resuscitation who are called to the scene of all arrests within the hospital.
This usually involves a specialized cart of equipment (including defibrillator) and drugs called a "crash cart" or "crash trolley".
Medical emergency teams – These teams respond to all emergencies, with the aim of treating the people in the acute phase of their illness in order to prevent a cardiac arrest. These teams have been found to decrease the rates of in hospital cardiac arrest and improve survival.[9]
Critical care outreach – As well as providing the services of the other two types of team, these teams are also responsible for educating non-specialist staff.
In addition, they help to facilitate transfers between intensive care/high dependency units and the general hospital wards. This is particularly important, as many studies have shown that a significant percentage of patients discharged from critical care environments quickly deteriorate and are re-admitted; the outreach team offers support to ward staff to prevent this from happening.
Implantable cardioverter defibrillator
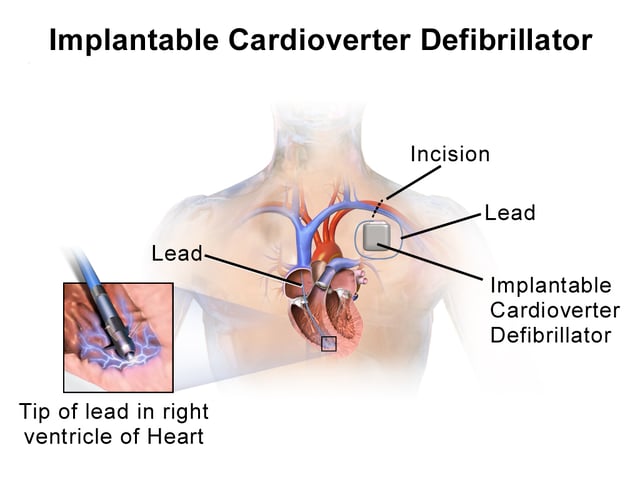
Illustration of implantable cardioverter defibrillator (ICD)
An implantable cardioverter defibrillator (ICD) is a battery powered device that monitors electrical activity in the heart and when an arrhythmia or asystole is detected is able to deliver an electrical shock to terminate the abnormal rhythm. ICDs are used to prevent sudden cardiac death (SCD) in those that have survived a prior episode of sudden cardiac arrest (SCA) due to ventricular fibrillation or ventricular tachycardia (secondary prevention).[49] ICD's are also used prophylactically to prevent sudden cardiac death in certain high risk patient populations (primary prevention).[50]
Numerous studies have been conducted on the use of ICDs for the secondary prevention of SCD.
These studies have shown improved survival with ICD's compared to the use of anti-arrhythmic drugs.[49] ICD therapy is associated with a 50% relative risk reduction in death caused by an arrhythmia and a 25% relative risk reduction in all cause mortality.[51]
Primary prevention of SCD with ICD therapy for high risk patient populations has similarly shown improved survival rates in a number of large studies.
The high risk patient populations in these studies were defined as those with severe ischemic cardiomyopathy (determined by a reduced left ventricular ejection fraction (LVEF)). The LVEF criteria used in these trials ranged from less than or equal to 30% in MADIT-II to less than or equal to 40% in MUSTT.[49][50]
Diet
Marine-derived omega-3 polyunsaturated fatty acids (PUFAs) have been promoted for the prevention of sudden cardiac death due to their postulated ability to lower triglyceride levels, prevent arrhythmias, decrease platelet aggregation, and lower blood pressure.[52] However, according to a recent systematic review, omega-3 PUFA supplementation are not being associated with a lower risk of sudden cardiac death.[53]
Management
Cardiopulmonary resuscitation
Early cardiopulmonary resuscitation (CPR) is essential to surviving cardiac arrest with good neurological function.[55] It is recommended that it be started as soon as possible with minimal interruptions once begun. The component of CPR that seems to make the greatest difference in most cases is the chest compressions. Correctly performed bystander CPR has been shown to increase survival; however, it is performed in less than 30% of out of hospital arrests as of 2007.[56] If high-quality CPR has not resulted in return of spontaneous circulation and the person's heart rhythm is in asystole, discontinuing CPR and pronouncing the person's death is reasonable after 20 minutes.[57] Exceptions to this include those with hypothermia or who have drowned.[57] Longer durations of CPR may be reasonable in those who have cardiac arrest while in hospital.[58] Bystander CPR, by the lay public, before the arrival of EMS also improves outcomes.[9]
Either a bag valve mask or an advanced airway may be used to help with breathing.[59] High levels of oxygen are generally given during CPR.[59] Tracheal intubation has not been found to improve survival rates or neurological outcome in cardiac arrest[56][60] and in the prehospital environment may worsen it.[61] Endotracheal tube and supraglottic airways appear equally useful.[60] When done by EMS 30 compressions followed by two breaths appear better than continuous chest compressions and breaths being given while compressions are ongoing.[62]
For bystanders, CPR which involves only chest compressions results in better outcomes as compared to standard CPR for those who have gone into cardiac arrest due to heart issues.[62] Mechanical chest compressions (as performed by a machine) are no better than chest compressions performed by hand.[59] It is unclear if a few minutes of CPR before defibrillation results in different outcomes than immediate defibrillation.[63] If cardiac arrest occurs after 20 weeks of pregnancy someone should pull or push the uterus to the left during CPR.[64] If a pulse has not returned by four minutes emergency Cesarean section is recommended.[64]
Defibrillation

An automated external defibrillator stored in a visible orange mural support
Defibrillation is indicated if a shockable rhythm is present.
The two shockable rhythms are ventricular fibrillation and pulseless ventricular tachycardia. In children 2 to 4 J/Kg is recommended.[65]
In addition, there is increasing use of public access defibrillation.
This involves placing an automated external defibrillator in public places, and training staff in these areas how to use them. This allows defibrillation to take place prior to the arrival of emergency services, and has been shown to lead to increased chances of survival. Some defibrillators even provide feedback on the quality of CPR compressions, encouraging the lay rescuer to press the person's chest hard enough to circulate blood.[66] In addition, it has been shown that those who have arrests in remote locations have worse outcomes following cardiac arrest.[67]
Medications
Lipid emulsion as used in cardiac arrest due to local anesthetic agents
As of 2016 medications other than epinephrine (adrenaline), while included in guidelines, have not been shown to improve survival to hospital discharge following out-of-hospital cardiac arrest. This includes the use of atropine, lidocaine, and amiodarone.[68][69][70][71][72] Epinephrine in adults, as of 2019, appears to improve survival but it is unclear if it improves neurologically normal survival.[73] It is generally recommended every five minutes.[59] Vasopressin overall does not improve or worsen outcomes compared to epinephrine.[59] The combination of epinephrine, vasopressin, and methylprednisolone appears to improve outcomes.[74] Some of the lack of long-term benefit may be related to delays in epinephrine use.[75] While evidence does not support its use in children, guidelines state its use is reasonable.[65] Lidocaine and amiodarone are also deemed reasonable in children with cardiac arrest who have a shockable rhythm.[59][65] The general use of sodium bicarbonate or calcium is not recommended.[59][76]
The 2010 guidelines from the American Heart Association no longer contain the recommendation for using atropine in pulseless electrical activity and asystole for want of evidence for its use.[77] Neither lidocaine nor amiodarone, in those who continue in ventricular tachycardia or ventricular fibrillation despite defibrillation, improves survival to hospital discharge but both equally improve survival to hospital admission.[78]
Thrombolytics when used generally may cause harm but may be of benefit in those with a confirmed pulmonary embolism as the cause of arrest.[79][64] Evidence for use of naloxone in those with cardiac arrest due to opioids is unclear but it may still be used.[64] In those with cardiac arrest due to local anesthetic, lipid emulsion may be used.[64]
Targeted temperature management
Cooling adults after cardiac arrest who have a return of spontaneous circulation (ROSC) but no return of consciousness improves outcomes.[11][12] This procedure is called targeted temperature management (previously known as therapeutic hypothermia). People are typically cooled for a 24-hour period, with a target temperature of 32–36 °C (90–97 °F).[59] There are a number of methods used to lower the body temperature, such as applying ice packs or cold-water circulating pads directly to the body, or infusing cold saline. This is followed by gradual rewarming over the next 12 to 24 hrs.[81]
Recent meta-analysis found that the use of therapeutic hypothermia after out-of-hospital cardiac arrest is associated with improved survival rates and better neurological outcomes.[11]
Do not resuscitate
Some people choose to avoid aggressive measures at the end of life.
A do not resuscitate order (DNR) in the form of an advance health care directive makes it clear that in the event of cardiac arrest, the person does not wish to receive cardiopulmonary resuscitation.[82] Other directives may be made to stipulate the desire for intubation in the event of respiratory failure or, if comfort measures are all that are desired, by stipulating that healthcare providers should "allow natural death".[83]
Chain of survival
Several organizations promote the idea of a chain of survival. The chain consists of the following "links":
Early recognition If possible, recognition of illness before the person develops a cardiac arrest will allow the rescuer to prevent its occurrence.
Early recognition that a cardiac arrest has occurred is key to survival for every minute a patient stays in cardiac arrest, their chances of survival drop by roughly 10%.[32]
Early CPR improves the flow of blood and of oxygen to vital organs, an essential component of treating a cardiac arrest.
In particular, by keeping the brain supplied with oxygenated blood, chances of neurological damage are decreased.
Early defibrillation is effective for the management of ventricular fibrillation and pulseless ventricular tachycardia[32]
Early advanced care
Early post-resuscitation care which may include percutaneous coronary intervention[84]
If one or more links in the chain are missing or delayed, then the chances of survival drop significantly.
These protocols are often initiated by a code blue, which usually denotes impending or acute onset of cardiac arrest or respiratory failure, although in practice, code blue is often called in less life-threatening situations that require immediate attention from a physician.
Other
Resuscitation with extracorporeal membrane oxygenation devices has been attempted with better results for in-hospital cardiac arrest (29% survival) than out-of-hospital cardiac arrest (4% survival) in populations selected to benefit most.[85] Cardiac catheterization in those who have survived an out-of-hospital cardiac arrest appears to improve outcomes although high quality evidence is lacking.[86] It is recommended that it is done as soon as possible in those who have had a cardiac arrest with ST elevation due to underlying heart problems.[59]
The precordial thump may be considered in those with witnessed, monitored, unstable ventricular tachycardia (including pulseless VT) if a defibrillator is not immediately ready for use, but it should not delay CPR and shock delivery or be used in those with unwitnessed out of hospital arrest.[87]
Prognosis
The overall chance of survival among those who have cardiac arrest outside hospital is 10%.[88][89] Among those who have an out-of-hospital cardiac arrest, 70% occur at home and their survival rate is 6%.[90][91] For those who have an in-hospital cardiac arrest, the survival rate is estimated to be 24%.[92] Among children rates of survival are 3 to 16% in North America.[65] For in hospital cardiac arrest survival to discharge is around 22% with many having a good neurological outcome.[9]
Prognosis is typically assessed 72 hours or more after cardiac arrest.[59] Rates of survival are better in those who someone saw collapse, got bystander CPR, or had either ventricular tachycardia or ventricular fibrillation when assessed.[96] Survival among those with Vfib or Vtach is 15 to 23%.[96] Women are more likely to survive cardiac arrest and leave hospital than men.[97]
A 1997 review found rates of survival to discharge of 14% although different studies varied from 0 to 28%.[98] In those over the age of 70 who have a cardiac arrest while in hospital, survival to hospital discharge is less than 20%.[99] How well these individuals are able to manage after leaving hospital is not clear.[99]
A study of survival rates from out-of-hospital cardiac arrest found that 14.6% of those who had received resuscitation by paramedics survived as far as admission to hospital.
Of these, 59% died during admission, half of these within the first 24 hours, while 46% survived until discharge from hospital.
This reflects an overall survival following cardiac arrest of 6.8%.
Of these 89% had normal brain function or mild neurological disability, 8.5% had moderate impairment, and 2% had major neurological disability.
Of those who were discharged from hospital, 70% were still alive four years later.[100]
Epidemiology
Based on death certificates, sudden cardiac death accounts for about 15% of all deaths in Western countries.[21] In the United States 326,000 cases of out of hospital and 209,000 cases of in hospital cardiac arrest occur among adults a year.[9] The lifetime risk is three times greater in men (12.3%) than women (4.2%) based on analysis of the Framingham Heart Study.[102] However this gender difference disappeared beyond 85 years of age.[21]
Society and culture
Names
In many publications the stated or implicit meaning of "sudden cardiac death" is sudden death from cardiac causes.[103] However, sometimes physicians call cardiac arrest "sudden cardiac death" even if the person survives. Thus one can hear mentions of "prior episodes of sudden cardiac death" in a living person.[104]
In 2006 the American Heart Association presented the following definitions of sudden cardiac arrest and sudden cardiac death: "Cardiac arrest is the sudden cessation of cardiac activity so that the victim becomes unresponsive, with no normal breathing and no signs of circulation.
If corrective measures are not taken rapidly, this condition progresses to sudden death.
Cardiac arrest should be used to signify an event as described above, that is reversed, usually by CPR and/or defibrillation or cardioversion, or cardiac pacing.
Sudden cardiac death should not be used to describe events that are not fatal".[105]
Show code
In some medical facilities, the resuscitation team may purposely respond slowly to a person in cardiac arrest, a practice known as "slow code", or may fake the response altogether for the sake of the person's family, a practice known as "show code".[106] This is generally done for people for whom performing CPR will have no medical benefit.[107] Such practices are ethically controversial,[108] and are banned in some jurisdictions.