Bipolar disorder

Bipolar disorder
| Bipolar disorder | |
|---|---|
| Other names | Bipolar affective disorder (BPAD),[1] bipolar illness, manic depression, manic depressive disorder, manic-depressive illness,[2] manic-depressive psychosis, circular insanity,[2] bipolar disease[3] |
| Bipolar disorder is characterized by episodes of depression and mania. | |
| Specialty | Psychiatry |
| Symptoms | Periods of depression and elevated mood[4][5] |
| Complications | Suicide, self-harm[4] |
| Usual onset | 25 years old[4] |
| Types | Bipolar I disorder, bipolar II disorder, others[5] |
| Causes | Environmental and genetic[4] |
| Risk factors | Family history, childhood abuse, long-term stress[4] |
| Differential diagnosis | Attention deficit hyperactivity disorder, personality disorders, schizophrenia, substance use disorder[4] |
| Treatment | Psychotherapy, medications[4] |
| Medication | Lithium, antipsychotics, anticonvulsants[4] |
| Frequency | 1–3%[4][6] |
Bipolar disorder, previously known as manic depression, is a mental disorder that causes periods of depression and abnormally elevated moods.[4][5][7] The elevated mood is significant and is known as mania, or hypomania if less severe and symptoms of psychosis are absent.[4] During mania, an individual behaves or feels abnormally energetic, happy, or irritable.[4] Individuals often make poorly thought out decisions with little regard to the consequences.[5] The need for sleep is usually reduced during manic phases.[5] During periods of depression, there may be crying, a negative outlook on life, and poor eye contact with others.[4] The risk of suicide among those with the illness is high at greater than 6 percent over 20 years, while self-harm occurs in 30–40 percent.[4] Other mental health issues such as anxiety disorders and substance use disorder are commonly associated with bipolar disorder.[4]
The causes are not clearly understood, but both environmental and genetic factors play a role.[4] Many genes, each with small effects, contribute to the disorder.[4][8] Environmental risk factors include a history of childhood abuse and long-term stress.[4] About 85% of the risk is attributed to genetics.[9] The condition is classified as bipolar I disorder if there has been at least one manic episode, with or without depressive episodes, and as bipolar II disorder if there has been at least one hypomanic episode (but no full manic episodes) and one major depressive episode.[5] In those with less severe symptoms of a prolonged duration, the condition cyclothymic disorder may be diagnosed.[5] If the symptoms are due to drugs or medical problems, it is classified separately.[5] Other conditions that may present similarly include attention deficit hyperactivity disorder, personality disorders, schizophrenia and substance use disorder as well as a number of medical conditions.[4] Medical testing is not required for a diagnosis, though blood tests or medical imaging can be done to rule out other problems.[10]
Bipolar disorder is treated with medications, such as mood stabilizers and antipsychotics, as well as with psychotherapy.[4][11] Mood stabilizers may improve mood disturbances, and include lithium and certain anticonvulsants such as valproate and carbamazepine.[4] Involuntary treatment in a psychiatric hospital may be needed if a person is a risk to themselves or others but refuses treatment.[4] Severe behavioral problems, such as agitation or combativeness, may be managed with short-term antipsychotics or benzodiazepines.[4] In periods of mania, it is recommended that antidepressants be stopped.[4] If antidepressants are used for periods of depression, they should be used with a mood stabilizer.[4] Electroconvulsive therapy (ECT), while not very well studied, may be tried for those who do not respond to other treatments.[4][12] If any treatment is stopped, it is recommended that this be done slowly.[4] Many individuals have financial, social or work-related problems due to the illness.[4] These difficulties occur a quarter to a third of the time, on average.[4] Due to lifestyle choices and the side effects of medications, the risk of death from natural causes such as coronary heart disease in people with bipolar is twice that of the general population.[4]
Bipolar disorder affects approximately 1% of the global population.[13] In the United States, about 3% are estimated to be affected at some point in their life; rates appear to be similar in females and males.[6][14] The most common age at which symptoms begin is 25.[4] The economic cost of the disorder has been estimated at $45 billion for the United States in 1991.[15] A large proportion of this was related to a higher number of missed work days, estimated at 50 per year.[15] People with bipolar disorder often face problems with social stigma.[4]
| Bipolar disorder | |
|---|---|
| Other names | Bipolar affective disorder (BPAD),[1] bipolar illness, manic depression, manic depressive disorder, manic-depressive illness,[2] manic-depressive psychosis, circular insanity,[2] bipolar disease[3] |
| Bipolar disorder is characterized by episodes of depression and mania. | |
| Specialty | Psychiatry |
| Symptoms | Periods of depression and elevated mood[4][5] |
| Complications | Suicide, self-harm[4] |
| Usual onset | 25 years old[4] |
| Types | Bipolar I disorder, bipolar II disorder, others[5] |
| Causes | Environmental and genetic[4] |
| Risk factors | Family history, childhood abuse, long-term stress[4] |
| Differential diagnosis | Attention deficit hyperactivity disorder, personality disorders, schizophrenia, substance use disorder[4] |
| Treatment | Psychotherapy, medications[4] |
| Medication | Lithium, antipsychotics, anticonvulsants[4] |
| Frequency | 1–3%[4][6] |
Signs and symptoms
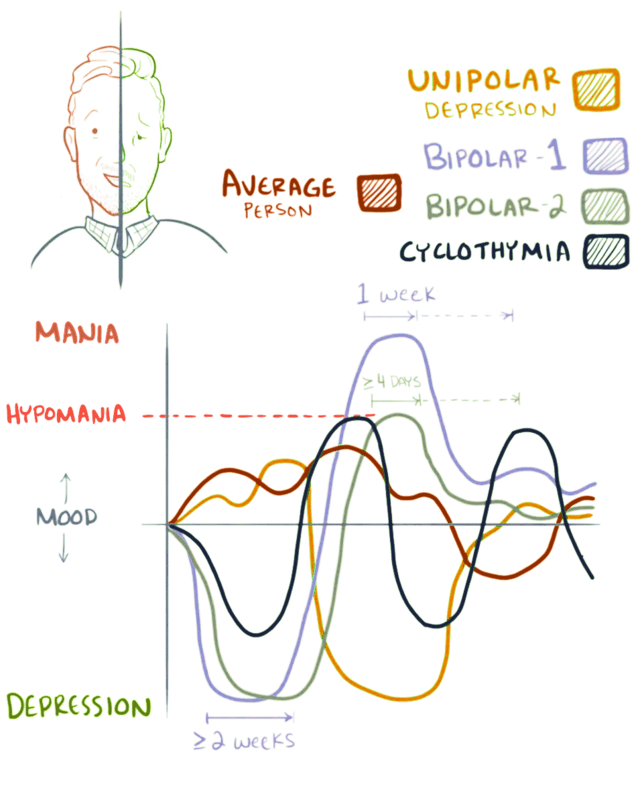
Bipolar mood shifts
Both mania and depression are characterized by disruptions in normal mood, psychomotor activity, circadian rhythm, and cognition. Mania can present with varying levels of mood disturbance, ranging from euphoria that is associated with "classic mania" to dysphoria and irritability. The core symptom of mania involves an increase in energy of psychomotor activity. Mania can also present with increased self-esteem or grandiosity, rapid speech, the subjective feeling of rapid thoughts, disinhibited social behavior, or impulsivity.[16] Mania is distinguished from hypomania by length, as hypomania requires four consecutive days, and mania requires more than a week. Unlike mania, hypomania is not always associated with impaired functioning.[13] The biological mechanisms responsible for switching from a manic or hypomanic episode to a depressive episode, or vice versa, remain poorly understood.[17]
Manic episodes

An 1892 color lithograph depicting a woman diagnosed with "Hilarious Mania"
Mania is a distinct period of at least one week of elevated or irritable mood, which can range from euphoria to delirium, and those experiencing hypomania or mania generally exhibit several of the following behaviors: speaking in a rapid, uninterruptible manner, decreased need for sleep, short attention span, racing thoughts, increased goal-oriented activities, agitation, or exhibition of behaviors characterized as impulsive or high-risk, such as hypersexuality or excessive spending.[18][19][20] To meet the definition for a manic episode, these behaviors must impair the individual's ability to socialize or work.[18][20] If untreated, a manic episode usually lasts three to six months.[21]
Manic individuals often have a history of substance abuse developed over years as a form of "self-medication".[22] At the most extreme, a person in a full-blown manic state can experience psychosis: a break with reality, a state in which thinking is affected along with mood.[20] They may feel unstoppable, or as if they have been "chosen" and are on a "special mission", or have other grandiose or delusional ideas.[23] This may lead to violent behavior and, sometimes, hospitalization in an inpatient psychiatric hospital.[19][20] The severity of manic symptoms can be measured by rating scales such as the Young Mania Rating Scale, though questions remain about the reliability of these scales.[24]
Hypomanic episodes
An 1858 lithograph captioned 'Melancholy passing into mania'
Hypomania is the milder form of mania, defined as at least four days of the same criteria as mania,[20] but which does not cause a significant decrease in the individual's ability to socialize or work, lacks psychotic features such as delusions or hallucinations, and does not require psychiatric hospitalization.[18] Overall functioning may actually increase during episodes of hypomania and is thought to serve as a defense mechanism against depression by some.[27] Hypomanic episodes rarely progress to full-blown manic episodes.[27] Some people who experience hypomania show increased creativity[20][28] while others are irritable or demonstrate poor judgment.
Hypomania may feel good to some persons who experience it, though most people who experience hypomania state that the stress of the experience is very painful.[20] Bipolar people who experience hypomania, however, tend to forget the effects of their actions on those around them. Even when family and friends recognize mood swings, the individual will often deny that anything is wrong.[29] What might be called a "hypomanic event", if not accompanied by depressive episodes, is often not deemed problematic, unless the mood changes are uncontrollable, or volatile.[27] Most commonly, symptoms continue for a few weeks to a few months.[30]
Depressive episodes
'Melancholy' by W. Bagg after a photograph by Hugh Welch Diamond
Symptoms of the depressive phase of bipolar disorder include persistent feelings of sadness, irritability or anger, loss of interest in previously enjoyed activities, excessive or inappropriate guilt, hopelessness, sleeping too much or not enough, changes in appetite and/or weight, fatigue, problems concentrating, self-loathing or feelings of worthlessness, and thoughts of death or suicide.[31] In severe cases, the individual may develop symptoms of psychosis, a condition also known as severe bipolar disorder with psychotic features. These symptoms include delusions and hallucinations. A major depressive episode persists for at least two weeks, and may result in suicide if left untreated.[32]
The earlier the age of onset, the more likely the first few episodes are to be depressive.[33] Since a diagnosis of bipolar disorder requires a manic or hypomanic episode, many affected individuals are initially misdiagnosed as having major depression and then incorrectly treated with prescribed antidepressants.[34]
Mixed affective episodes
In bipolar disorder, mixed state is a condition during which symptoms of both mania and depression occur simultaneously.[35] Individuals experiencing a mixed state may have manic symptoms such as grandiose thoughts while simultaneously experiencing depressive symptoms such as excessive guilt or feeling suicidal.[35] Mixed states are considered to be high-risk for suicidal behavior since depressive emotions such as hopelessness are often paired with mood swings or difficulties with impulse control.[35] Anxiety disorders occur more frequently as a comorbidity in mixed bipolar episodes than in non-mixed bipolar depression or mania.[35] Substance abuse (including alcohol) also follows this trend, thereby appearing to depict bipolar symptoms as no more than a consequence of substance abuse.[35]
Associated features
Associated features are clinical phenomena that often accompany the disorder but are not part of the diagnostic criteria. In adults with the condition, bipolar disorder is often accompanied by changes in cognitive processes and abilities.[36] These include reduced attentional and executive capabilities and impaired memory.[37] How the individual processes the universe also depends on the phase of the disorder, with differential characteristics between the manic, hypomanic and depressive states.[26] Those with bipolar disorder may have difficulty in maintaining relationships.[38] There are several common childhood precursors seen in children who later receive a diagnosis of bipolar disorder, such as mood abnormalities (including major depressive episodes) and attention deficit hyperactivity disorder (ADHD).[39]
Comorbid conditions
The diagnosis of bipolar disorder can be complicated by coexisting (comorbid) psychiatric conditions including the following: obsessive-compulsive disorder, substance-use disorder, eating disorders, attention deficit hyperactivity disorder, social phobia, premenstrual syndrome (including premenstrual dysphoric disorder), or panic disorder.[22][31][40][41] A careful longitudinal analysis of symptoms and episodes, enriched if possible by discussions with friends and family members, is crucial to establishing a treatment plan where these comorbidities exist.[42]
Causes
The causes of bipolar disorder likely vary between individuals and the exact mechanism underlying the disorder remains unclear.[43] Genetic influences are believed to account for 60–80 percent of the risk of developing the disorder indicating a strong hereditary component.[40] The overall heritability of the bipolar spectrum has been estimated at 0.71.[44] Twin studies have been limited by relatively small sample sizes but have indicated a substantial genetic contribution, as well as environmental influence. For bipolar disorder type I, the rate at which identical twins (same genes) will both have bipolar disorder type I (concordance) is estimated at around 40 percent, compared to about 5 percent in fraternal twins.[18][45] A combination of bipolar I, II, and cyclothymia similarly produced rates of 42 percent and 11 percent (identical and fraternal twins, respectively), with a relatively lower ratio for bipolar II that likely reflects heterogeneity. There is overlap with major (unipolar) depression and if this is also counted in the co-twin the concordance with bipolar disorder rises to 67 percent in identical twins and 19 percent in fraternal twins.[46] The relatively low concordance between fraternal twins brought up together suggests that shared family environmental effects are limited, although the ability to detect them has been limited by small sample sizes.[44] Estrogen in women has been linked to bipolar disorder.[47][48]
Genetic
Behavioral genetic studies have suggested that many chromosomal regions and candidate genes are related to bipolar disorder susceptibility with each gene exerting a mild to moderate effect.[40] The risk of bipolar disorder is nearly ten-fold higher in first degree-relatives of those affected with bipolar disorder when compared to the general population; similarly, the risk of major depressive disorder is three times higher in relatives of those with bipolar disorder when compared to the general population.[18]
Although the first genetic linkage finding for mania was in 1969,[49] the linkage studies have been inconsistent.[18] The largest and most recent genome-wide association study (GWAS) failed to find any particular locus that exerts a large effect, reinforcing the idea that no single gene is responsible for bipolar disorder in most cases.[50] Polymorphisms in BDNF, DRD4, DAO, and TPH1 have been frequently associated with bipolar disorder and were initially successful in a meta-analysis, but failed after correction for multiple testing.[51] On the other hand, two polymorphisms in TPH2 were identified as being associated with bipolar disorder.[52]
Due to the inconsistent findings in a genome-wide association study, multiple studies have undertaken the approach of analyzing single-nucleotide polymorphisms (SNPs) in biological pathways. Signaling pathways traditionally associated with bipolar disorder that have been supported by these studies include corticotropin-releasing hormone (CRH) signaling, cardiac β-adrenergic signaling, Phospholipase C signaling, glutamate receptor signaling,[53] cardiac hypertrophy signaling, Wnt signaling, Notch signaling,[54] and endothelin 1 signaling. Of the 16 genes identified in these pathways, three were found to be dysregulated in the dorsolateral prefrontal cortex portion of the brain in post-mortem studies, CACNA1C, GNG2, and ITPR2.[55]
Bipolar disorder is associated with reduced expression of specific DNA repair enzymes and increased levels of oxidative DNA damages.[57]
Advanced paternal age has been linked to a somewhat increased chance of bipolar disorder in offspring, consistent with a hypothesis of increased new genetic mutations.[58]
Environmental
Psychosocial factors play a significant role in the development and course of bipolar disorder, and individual psychosocial variables may interact with genetic dispositions.[59] It is probable that recent life events and interpersonal relationships contribute to the onset and recurrence of bipolar mood episodes, just as they do for unipolar depression.[60] In surveys, 30–50 percent of adults diagnosed with bipolar disorder report traumatic/abusive experiences in childhood, which is associated with earlier onset, a higher rate of suicide attempts, and more co-occurring disorders such as post-traumatic stress disorder (PTSD).[61] The number of reported stressful events in childhood is higher in those with an adult diagnosis of bipolar spectrum disorder compared to those without, particularly events stemming from a harsh environment rather than from the child's own behavior.[62]
Neurological
Less commonly, bipolar disorder or a bipolar-like disorder may occur as a result of or in association with a neurological condition or injury. Conditions like these and injuries include stroke, traumatic brain injury, HIV infection, multiple sclerosis, porphyria, and rarely temporal lobe epilepsy.[63]
Mechanism
Physiological
Brain imaging studies have revealed differences in the volume of various brain regions between patients with bipolar disorder and healthy control subjects
Abnormalities in the structure and/or function of certain brain circuits could underlie bipolar disorder. Meta-analyses of structural MRI studies in bipolar disorder report decreased volume in the left rostral anterior cingulate cortex (ACC), fronto-insular cortex, ventral prefrontal cortex, and claustrum. Increases have been reported in the volume of the lateral ventricles, globus pallidus, subgenual anterior cingulate, and amygdala as well as in the rates of deep white matter hyperintensities.[64][65][66][67] Functional MRI findings suggest that abnormal modulation between ventral prefrontal and limbic regions, especially the amygdala, likely contributes to poor emotional regulation and mood symptoms.[68] Pharmacological treatment of mania increases ventral prefrontal cortex (vPFC) activity, normalizing it relative to controls, suggesting that vPFC hypoactivity is an indicator of mood state. On the other hand, pretreatment hyperactivity in the amygdala is reduced post-treatment but is still increased relative to controls, suggesting that it is a trait marker.[69]
Manic and depressive episodes tend to be characterized by ventral versus dorsal dysfunction in the ventral prefrontal cortex. During attentional tasks and resting, mania is associated with decreased orbitofrontal cortex activity, while depression is associated with increased resting metabolism. Consistent with affective disorders due to lesions, mania and depression are lateralized in vPFC dysfunction, with depression primarily being associated with the left vPFC, and mania the right vPFC. Abnormal vPFC activity, along with amygdala hyperactivity is found during euthymia as well as in healthy relatives of those with bipolar, indicating possible trait features.[70]
Euthymic bipolar people show decreased activity in the lingual gyrus, while people who are manic demonstrate decreased activity in the inferior frontal cortex, while no differences were found in people with bipolar depression.[71] People with bipolar have increased activation of left hemisphere ventral limbic areas and decreased activation of right hemisphere cortical structures related to cognition.[72]
One proposed model for bipolar disorder suggests that hypersensitivity of reward circuits consisting of frontostriatal circuits causes mania, and hyposensitivity of these circuits causes depression.[73]
According to the "kindling" hypothesis, when people who are genetically predisposed toward bipolar disorder experience stressful events, the stress threshold at which mood changes occur becomes progressively lower, until the episodes eventually start (and recur) spontaneously. There is evidence supporting an association between early-life stress and dysfunction of the hypothalamic-pituitary-adrenal axis (HPA axis) leading to its overactivation, which may play a role in the pathogenesis of bipolar disorder.[74][75]
Neurochemical
Dopamine, a known neurotransmitter responsible for mood cycling, has been shown to have increased transmission during the manic phase.[17][78] The dopamine hypothesis states that the increase in dopamine results in secondary homeostatic downregulation of key systems and receptors such as an increase in dopamine-mediated G protein-coupled receptors. This results in decreased dopamine transmission characteristic of the depressive phase.[17] The depressive phase ends with homeostatic up regulation potentially restarting the cycle over again.[79]
Glutamate is significantly increased within the left dorsolateral prefrontal cortex during the manic phase of bipolar disorder, and returns to normal levels once the phase is over.[80] The increase in gamma-Aminobutyric acid (GABA) is possibly caused by a disturbance in early development causing a disturbance of cell migration and the formation of normal lamination, the layering of brain structures commonly associated with the cerebral cortex.[81]
Medications used to treat bipolar may exert their effect by modulating intracellular signaling, such as through depleting myo-inositol levels, inhibition of cAMP signaling, and through altering G coupled proteins.[82] Consistent with this, elevated levels of Gαi, Gαs, and Gαq/11 have been reported in brain and blood samples, along with increased protein kinase A expression and sensitivity.[83]
Decreased levels of 5-hydroxyindoleacetic acid, a byproduct of serotonin, are present in the cerebrospinal fluid of persons with bipolar disorder during both the depressed and manic phases. Increased dopaminergic activity has been hypothesized in manic states due to the ability of dopamine agonists to stimulate mania in people with bipolar disorder. Decreased sensitivity of regulatory α2 adrenergic receptors as well as increased cell counts in the locus ceruleus indicated increased noradrenergic activity in manic people. Low plasma GABA levels on both sides of the mood spectrum have been found.[84] One review found no difference in monoamine levels, but found abnormal norepinephrine turnover in people with bipolar disorder.[85] Tyrosine depletion was found to reduce the effects of methamphetamine in people with bipolar disorder as well as symptoms of mania, implicating dopamine in mania. VMAT2 binding was found to be increased in one study of people with bipolar mania.[86]
Diagnosis
Bipolar disorder is commonly diagnosed during adolescence or early adulthood, but onset can occur throughout the life cycle.[5][87] The disorder can be difficult to distinguish from unipolar depression and the average delay in diagnosis is 5–10 years after symptoms begin.[88] Diagnosis of bipolar disorder takes several factors into account and considers the self-reported experiences of the symptomatic individual, abnormal behavior reported by family members, friends or co-workers, observable signs of illness as assessed by a clinician, and often a medical work-up to rule-out medical causes. In diagnosis, caregiver-scored rating scales, specifically the mother, has been found to be more accurate than teacher and youth report in predicting identifying youths with bipolar disorder.[89] Assessment is usually done on an outpatient basis; admission to an inpatient facility is considered if there is a risk to oneself or others. The most widely used criteria for diagnosing bipolar disorder are from the American Psychiatric Association's (APA) Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and the World Health Organization's (WHO) International Statistical Classification of Diseases and Related Health Problems, 10th Edition (ICD-10). The ICD-10 criteria are used more often in clinical settings outside of the U.S. while the DSM criteria are used clinically within the U.S. and are the prevailing criteria used internationally in research studies. The DSM-5, published in 2013, included further and more accurate specifiers compared to its predecessor, the DSM-IV-TR.[90] Semi structured interviews such as the Kiddie Schedule for Affective Disorders and Schizophrenia (KSADS) and the Structured Clinical Interview for DSM-IV (SCID) are used for diagnostic confirmation of bipolar disorder.
Several rating scales for the screening and evaluation of bipolar disorder exist,[91] including the Bipolar spectrum diagnostic scale, Mood Disorder Questionnaire, the General Behavior Inventory and the Hypomania Checklist.[92] The use of evaluation scales cannot substitute a full clinical interview but they serve to systematize the recollection of symptoms.[92] On the other hand, instruments for screening bipolar disorder tend to have lower sensitivity.[91]
Differential diagnosis
There are several other mental disorders with symptoms similar to those seen in bipolar disorder. These disorders include schizophrenia, major depressive disorder,[93] attention deficit hyperactivity disorder (ADHD), and certain personality disorders, such as borderline personality disorder.[94][95][96]
Although there are no biological tests that are diagnostic of bipolar disorder,[50] blood tests and/or imaging may be carried out to exclude medical illnesses with clinical presentations similar to that of bipolar disorder. Neurologic diseases such as multiple sclerosis, complex partial seizures, strokes, brain tumors, Wilson's disease, traumatic brain injury, Huntington's disease, and complex migraines can mimic features of bipolar disorder.[87] An EEG may be used to exclude neurological disorders such as epilepsy, and a CT scan or MRI of the head may be used to exclude brain lesions.[87] Additionally, disorders of the endocrine system such as hypothyroidism, hyperthyroidism, and Cushing's disease are in the differential as is the connective tissue disease systemic lupus erythematosus. Infectious causes of mania that may appear similar to bipolar mania include herpes encephalitis, HIV, influenza, or neurosyphilis.[87] Certain vitamin deficiencies such as pellagra (niacin deficiency), Vitamin B12 deficiency, folate deficiency, and Wernicke Korsakoff syndrome (thiamine deficiency) can also lead to mania.[87]
A review of current and recent medications and drug use is considered to rule out these causes; common medications that can cause manic symptoms include antidepressants, prednisone, Parkinson's disease medications, thyroid hormone, stimulants (including cocaine and methamphetamine), and certain antibiotics.[97]
Bipolar spectrum

Since Emil Kraepelin's distinction between bipolar disorder and schizophrenia in the 19th century, researchers have defined a spectrum of different types of bipolar disorder
Bipolar spectrum disorders includes: bipolar I disorder, bipolar II disorder, cyclothymic disorder and cases where subthreshold symptoms are found to cause clinically significant impairment or distress.[5][87] These disorders involve major depressive episodes that alternate with manic or hypomanic episodes, or with mixed episodes that feature symptoms of both mood states.[5] The concept of the bipolar spectrum is similar to that of Emil Kraepelin's original concept of manic depressive illness.[98]
Unipolar hypomania without accompanying depression has been noted in the medical literature.[99] There is speculation as to whether this condition may occur with greater frequency in the general, untreated population; successful social function of these potentially high-achieving individuals may lead to being labeled as normal, rather than as individuals with substantial dysregulation.
Criteria and subtypes

The DSM and the ICD characterize bipolar disorder as a spectrum of disorders occurring on a continuum. The DSM-5 lists three specific subtypes:[5]
Bipolar I disorder: At least one manic episode is necessary to make the diagnosis;[102] depressive episodes are common in the vast majority of cases with bipolar disorder I, but are unnecessary for the diagnosis.[18] Specifiers such as "mild, moderate, moderate-severe, severe" and "with psychotic features" should be added as applicable to indicate the presentation and course of the disorder.[5]
Bipolar II disorder: No manic episodes and one or more hypomanic episodes and one or more major depressive episode.[102] Hypomanic episodes do not go to the full extremes of mania (i.e., do not usually cause severe social or occupational impairment, and are without psychosis), and this can make bipolar II more difficult to diagnose, since the hypomanic episodes may simply appear as periods of successful high productivity and are reported less frequently than a distressing, crippling depression.
Cyclothymia: A history of hypomanic episodes with periods of depression that do not meet criteria for major depressive episodes.[103]
When relevant, specifiers for peripartum onset and with rapid cycling should be used with any subtype. Individuals who have subthreshold symptoms that cause clinically significant distress or impairment, but do not meet full criteria for one of the three subtypes may be diagnosed with other specified or unspecified bipolar disorder. Other specified bipolar disorder is used when a clinician chooses to provide an explanation for why the full criteria were not met (e.g., hypomania without a prior major depressive episode).[5]
Rapid cycling
Most people who meet criteria for bipolar disorder experience a number of episodes, on average 0.4 to 0.7 per year, lasting three to six months.[104] Rapid cycling, however, is a course specifier that may be applied to any of the above subtypes. It is defined as having four or more mood disturbance episodes within a one-year span and is found in a significant proportion of individuals with bipolar disorder.[31] These episodes are separated from each other by a remission (partial or full) for at least two months or a switch in mood polarity (i.e., from a depressive episode to a manic episode or vice versa).[18] The definition of rapid cycling most frequently cited in the literature (including the DSM) is that of Dunner and Fieve: at least four major depressive, manic, hypomanic or mixed episodes are required to have occurred during a 12-month period.[105] Ultra-rapid (days) and ultra-ultra rapid or ultradian (within a day) cycling have also been described.[106] The literature examining the pharmacological treatment of rapid cycling is sparse and there is no clear consensus with respect to its optimal pharmacological management.[107]
Prevention
Attempts at prevention of bipolar disorder have focused on stress (such as childhood adversity or highly conflictual families) which, although not a diagnostically specific causal agent for bipolar, does place genetically and biologically vulnerable individuals at risk for a more severe course of illness.[108] There has been debate regarding the causal relationship between usage of cannabis and bipolar disorder.[109]
Management
There are a number of pharmacological and psychotherapeutic techniques used to treat bipolar disorder. Individuals may use self-help and pursue recovery.
Hospitalization may be required especially with the manic episodes present in bipolar I. This can be voluntary or (local legislation permitting) involuntary (called civil or involuntary commitment). Long-term inpatient stays are now less common due to deinstitutionalization, although these can still occur.[110] Following (or in lieu of) a hospital admission, support services available can include drop-in centers, visits from members of a community mental health team or an Assertive Community Treatment team, supported employment and patient-led support groups, intensive outpatient programs. These are sometimes referred to as partial-inpatient programs.[111]
Psychosocial
Psychotherapy is aimed at alleviating core symptoms, recognizing episode triggers, reducing negative expressed emotion in relationships, recognizing prodromal symptoms before full-blown recurrence, and, practicing the factors that lead to maintenance of remission.[112][113][114] Cognitive behavioral therapy, family-focused therapy, and psychoeducation have the most evidence for efficacy in regard to relapse prevention, while interpersonal and social rhythm therapy and cognitive-behavioral therapy appear the most effective in regard to residual depressive symptoms. Most studies have been based only on bipolar I, however, and treatment during the acute phase can be a particular challenge.[115] Some clinicians emphasize the need to talk with individuals experiencing mania, to develop a therapeutic alliance in support of recovery.[116]
Medication
Lithium is often used to treat bipolar disorder and has the best evidence for reducing suicide.
A number of medications are used to treat bipolar disorder.[60] The medication with the best evidence is lithium, which is an effective treatment for acute manic episodes, preventing relapses, and bipolar depression.[117] Lithium reduces the risk of suicide, self-harm, and death in people with bipolar disorder.[118] It is unclear if ketamine (a common general dissociative anesthetic used in surgery) is useful in bipolar as of 2015.[119]
Mood stabilizers
Lithium and the anticonvulsants carbamazepine, lamotrigine, and valproic acid are used as mood stabilizers to treat bipolar disorder. These mood stabilizers are used for long-term mood stabilization but have not demonstrated the ability to quickly treat acute bipolar depression.[120] Lithium is preferred for long-term mood stabilization.[60] Carbamazepine effectively treats manic episodes, with some evidence it has greater benefit in rapid-cycling bipolar disorder, or those with more psychotic symptoms or a more schizoaffective clinical picture. It is less effective in preventing relapse than lithium or valproate.[121][122] Valproate has become a commonly prescribed treatment and effectively treats manic episodes.[123] Lamotrigine has some efficacy in treating bipolar depression, and this benefit is greatest in more severe depression.[124] It has also been shown to have some benefit in preventing bipolar disorder relapses, though there are concerns about the studies done, and is of no benefit in rapid cycling subtype of bipolar disorder.[125] The effectiveness of topiramate is unknown.[126]
Antipsychotics
Antipsychotic medications are effective for short-term treatment of bipolar manic episodes and appear to be superior to lithium and anticonvulsants for this purpose.[60] Atypical antipsychotics are also indicated for bipolar depression refractory to treatment with mood stabilizers.[120] Olanzapine is effective in preventing relapses, although the supporting evidence is weaker than the evidence for lithium.[127]
Antidepressants
Antidepressants are not recommended for use alone in the treatment of bipolar disorder and have not been found to be of any benefit over that found with mood stabilizers.[13][128] Atypical antipsychotic medications (e.g., aripiprazole) are preferred over antidepressants to augment the effects of mood stabilizers due to the lack of efficacy of antidepressants in bipolar disorder.[120]
Other
Short courses of benzodiazepines may be used in addition to other medications until mood stabilizing become effective.[129] Electroconvulsive therapy (ECT) is an effective form of treatment for acute mood disturbances in those with bipolar disorder, especially when psychotic or catatonic features are displayed.[13] ECT is also recommended for use in pregnant women with bipolar disorder.[13]
Contrary to widely held views, stimulants are relatively safe in bipolar disorder, and considerable evidence suggests they may even produce an antimanic effect. In cases of comorbid ADHD and bipolar, stimulants may help improve both conditions.[130]
Alternative medicine
Prognosis
A lifelong condition with periods of partial or full recovery in between recurrent episodes of relapse,[31][131] bipolar disorder is considered to be a major health problem worldwide because of the increased rates of disability and premature mortality.[131] It is also associated with co-occurring psychiatric and medical problems, and high rates of initial under- or misdiagnosis, causing a delay in appropriate treatment interventions and contributing to poorer prognoses.[33] After a diagnosis is made, it remains difficult to achieve complete remission of all symptoms with the currently available psychiatric medications and symptoms often become progressively more severe over time.[91][133]
Compliance with medications is one of the most significant factors that can decrease the rate and severity of relapse and have a positive impact on overall prognosis.[134] However, the types of medications used in treating BD commonly cause side effects[135] and more than 75% of individuals with BD inconsistently take their medications for various reasons.[134]
Of the various types of the disorder, rapid cycling (four or more episodes in one year) is associated with the worst prognosis due to higher rates of self-harm and suicide.[31] Individuals diagnosed with bipolar who have a family history of bipolar disorder are at a greater risk for more frequent manic/hypomanic episodes.[136] Early onset and psychotic features are also associated with worse outcomes,[137][138] as well as subtypes that are nonresponsive to lithium.[133]
Early recognition and intervention also improve prognosis as the symptoms in earlier stages are less severe and more responsive to treatment.[133] Onset after adolescence is connected to better prognoses for both genders, and being male is a protective factor against higher levels of depression. For women, better social functioning prior to developing bipolar disorder and being a parent are protective towards suicide attempts.[136]
Functioning
People with bipolar disorder often experience a decline in cognitive functioning during (or possibly before) their first episode, after which a certain degree of cognitive dysfunction typically becomes permanent, with more severe impairment during acute phases and moderate impairment during periods of remission. As a result, two-thirds of people with BD continue to experience impaired psychosocial functioning in between episodes even when their mood symptoms are in full remission. A similar pattern is seen in both BD-I and BD-II, but people with BD-II experience a lesser degree of impairment.[135] Cognitive deficits typically increase over the course of the illness. Higher degrees of impairment correlate with the number of previous manic episodes and hospitalizations, and with the presence of psychotic symptoms.[139] Early intervention can slow the progression of cognitive impairment, while treatment at later stages can help reduce distress and negative consequences related to cognitive dysfunction.[133]
Despite the overly ambitious goals that are frequently part of manic episodes, symptoms of mania undermine the ability to achieve these goals and often interfere with an individual's social and occupational functioning. One third of people with BD remain unemployed for one year following a hospitalization for mania.[140] Depressive symptoms during and between episodes, which occur much more frequently for most people than hypomanic or manic symptoms over the course of illness, are associated with lower functional recovery in between episodes, including unemployment or underemployment for both BD-I and BD-II.[5][141] However, the course of illness (duration, age of onset, number of hospitalizations, and presence or not of rapid cycling) and cognitive performance are the best predictors of employment outcomes in individuals with bipolar disorder, followed by symptoms of depression and years of education.[141]
Recovery and recurrence
A naturalistic study from first admission for mania or mixed episode (representing the hospitalized and therefore most severe cases) found that 50 percent achieved syndromal recovery (no longer meeting criteria for the diagnosis) within six weeks and 98 percent within two years. Within two years, 72 percent achieved symptomatic recovery (no symptoms at all) and 43 percent achieved functional recovery (regaining of prior occupational and residential status). However, 40 percent went on to experience a new episode of mania or depression within 2 years of syndromal recovery, and 19 percent switched phases without recovery.[142]
Suicide
Bipolar disorder can cause suicidal ideation that leads to suicidal attempts. Individuals whose bipolar disorder begins with a depressive or mixed affective episode seem to have a poorer prognosis and an increased risk of suicide.[93] One out of two people with bipolar disorder attempt suicide at least once during their lifetime and many attempts are successfully completed.[40] The annual average suicide rate is 0.4 percent, which is 10–20 times that of the general population.[145] The standardized mortality ratio from suicide in bipolar disorder is between 18 and 25.[146] The lifetime risk of suicide has been estimated to be as high as 20 percent in those with bipolar disorder.[18]
Epidemiology

Burden of bipolar disorder around the world: disability-adjusted life years per 100,000 inhabitants in 2004. <180 180–185 185–190 190–195 195–200 200–205 205–210 210–215 215–220 220–225 225–230 >230
Bipolar disorder is the sixth leading cause of disability worldwide and has a lifetime prevalence of about 1 to 3 percent in the general population.[6][147][148] However, a reanalysis of data from the National Epidemiological Catchment Area survey in the United States suggested that 0.8 percent of the population experience a manic episode at least once (the diagnostic threshold for bipolar I) and a further 0.5 percent have a hypomanic episode (the diagnostic threshold for bipolar II or cyclothymia). Including sub-threshold diagnostic criteria, such as one or two symptoms over a short time-period, an additional 5.1 percent of the population, adding up to a total of 6.4 percent, were classified as having a bipolar spectrum disorder.[149] A more recent analysis of data from a second US National Comorbidity Survey found that 1 percent met lifetime prevalence criteria for bipolar I, 1.1 percent for bipolar II, and 2.4 percent for subthreshold symptoms.[150]
There are conceptual and methodological limitations and variations in the findings. Prevalence studies of bipolar disorder are typically carried out by lay interviewers who follow fully structured/fixed interview schemes; responses to single items from such interviews may suffer limited validity. In addition, diagnoses (and therefore estimates of prevalence) vary depending on whether a categorical or spectrum approach is used. This consideration has led to concerns about the potential for both underdiagnosis and overdiagnosis.[151]
The incidence of bipolar disorder is similar in men and women[152] as well as across different cultures and ethnic groups.[153] A 2000 study by the World Health Organization found that prevalence and incidence of bipolar disorder are very similar across the world. Age-standardized prevalence per 100,000 ranged from 421.0 in South Asia to 481.7 in Africa and Europe for men and from 450.3 in Africa and Europe to 491.6 in Oceania for women. However, severity may differ widely across the globe. Disability-adjusted life year rates, for example, appear to be higher in developing countries, where medical coverage may be poorer and medication less available.[154] Within the United States, Asian Americans have significantly lower rates than their African and European American counterparts.[155]
History
German psychiatrist Emil Kraepelin first distinguished between manic–depressive illness and "dementia praecox" (now known as schizophrenia) in the late 19th century
Variations in moods and energy levels have been observed as part of the human experience throughout history. The words "melancholia", an old word for depression, and "mania" originated in Ancient Greece. The word melancholia is derived from melas (μέλας), meaning "black", and chole (χολή), meaning "bile" or "gall",[159] indicative of the term's origins in pre-Hippocratic humoral theory. Within the humoral theories, mania was viewed as arising from an excess of yellow bile, or a mixture of black and yellow bile. The linguistic origins of mania, however, are not so clear-cut. Several etymologies were proposed by the Ancient Roman physician Caelius Aurelianus, including the Greek word ania, meaning "to produce great mental anguish", and manos, meaning "relaxed" or "loose", which would contextually approximate to an excessive relaxing of the mind or soul.[160] There are at least five other candidates, and part of the confusion surrounding the exact etymology of the word mania is its varied usage in the pre-Hippocratic poetry and mythology.[160]
In the early 1800s, French psychiatrist Jean-Étienne Dominique Esquirol's lypemania, one of his affective monomanias, was the first elaboration on what was to become modern depression.[161] The basis of the current conceptualisation of bipolar illness can be traced back to the 1850s; In 1850, Jean-Pierre Falret presented a description to the Academy the Paris Psychiatric Society in the course of which he mentioned "circular insanity" (la folie circulaire, French pronunciation: [la fɔli siʁ.ky.lɛʁ]); the lecture was summarized in 1851 in the "Gazette des hôpitaux" ("Hospital Gazette").[2] Three years later, in 1854, Jules-Gabriel-François Baillarger (1809–1890) described to the French Imperial Académie Nationale de Médecine a biphasic mental illness causing recurrent oscillations between mania and melancholia, which he termed folie à double forme (French pronunciation: [fɔli a dubl fɔʀm], "madness in double form").[2][162] Baillarger's original paper, "De la folie à double forme," appeared in the medical journal Annales médico-psychologiques (Medico-psychological annals) in 1854.[2]
These concepts were developed by the German psychiatrist Emil Kraepelin (1856–1926), who, using Kahlbaum's concept of cyclothymia,[163] categorized and studied the natural course of untreated bipolar patients. He coined the term manic depressive psychosis, after noting that periods of acute illness, manic or depressive, were generally punctuated by relatively symptom-free intervals where the patient was able to function normally.[164]
The term "manic–depressive reaction" appeared in the first version of the DSM in 1952, influenced by the legacy of Adolf Meyer.[165] Subtyping into "unipolar" depressive disorders and bipolar disorders has its origin in Karl Kleist's concept – since 1911 – of unipolar and bipolar affective disorders, which was used by Karl Leonhard in 1957 to differentiate between unipolar and bipolar disorder in depression.[160] These subtypes have been regarded as separate conditions since publication of the DSM-III. The subtypes bipolar II and rapid cycling have been included since the DSM-IV, based on work from the 1970s by David Dunner, Elliot Gershon, Frederick Goodwin, Ronald Fieve, and Joseph Fleiss.[166][167][168]
Society and culture

Singer Rosemary Clooney's public revelation of bipolar disorder made her an early celebrity spokeswoman for mental illness.[169]
There are widespread problems with social stigma, stereotypes, and prejudice against individuals with a diagnosis of bipolar disorder.[170]
Kay Redfield Jamison, a clinical psychologist and professor of psychiatry at the Johns Hopkins University School of Medicine, profiled her own bipolar disorder in her memoir An Unquiet Mind (1995).[171] In his autobiography Manicdotes: There's Madness in His Method (2008), Chris Joseph describes his struggle between the creative dynamism which allowed the creation of his multimillion-pound advertising agency Hook Advertising, and the money-squandering dark despair of his bipolar illness.[172]
Several dramatic works have portrayed characters with traits suggestive of the diagnosis that has been the subject of discussion by psychiatrists and film experts alike. A notable example is Mr. Jones (1993), in which Mr. Jones (Richard Gere) swings from a manic episode into a depressive phase and back again, spending time in a psychiatric hospital and displaying many of the features of the syndrome.[173] In The Mosquito Coast (1986), Allie Fox (Harrison Ford) displays some features including recklessness, grandiosity, increased goal-directed activity and mood lability, as well as some paranoia.[174] Psychiatrists have suggested that Willy Loman, the main character in Arthur Miller's classic play Death of a Salesman, suffers from bipolar disorder,[175] though that specific term for the condition did not exist when the play was written.
TV specials, for example the BBC's Stephen Fry: The Secret Life of the Manic Depressive,[176] MTV's True Life: I'm Bipolar, talk shows, and public radio shows, and the greater willingness of public figures to discuss their own bipolar disorder, have focused on psychiatric conditions, thereby, raising public awareness.
On April 7, 2009, the nighttime drama 90210 on the CW network, aired a special episode where the character Silver was diagnosed with bipolar disorder.[177] Stacey Slater, a character from the BBC soap EastEnders, has been diagnosed with the disorder. The storyline was developed as part of the BBC's Headroom campaign.[178] The Channel 4 soap Brookside had earlier featured a story about bipolar disorder when the character Jimmy Corkhill was diagnosed with the condition.[179] 2011 Showtime's political thriller drama Homeland protagonist Carrie Mathison is bipolar, which she has kept secret since her school days.[180] In April 2014, ABC premiered a medical drama, Black Box, in which the main character, a world-renowned neuroscientist, is bipolar.[181]
In an effort to ease the social stigma associated with bipolar disorder, the orchestra conductor Ronald Braunstein cofounded the ME/2 Orchestra with his wife Caroline Whiddon in 2011. Braunstein was diagnosed with bipolar disorder in 1985 and his concerts with the ME/2 Orchestra were conceived in order to create a welcoming performance environment for his musical colleagues, while also raising public awareness about mental illness.[182][183]
Creativity
A link between mental illness and professional success or creativity has been suggested, including in accounts by Socrates, Seneca the Younger, and Cesare Lombroso. Despite prominence in popular culture, the link between creativity and bipolar has not been rigorously studied. This area of study also is likely affected by confirmation bias. Some evidence suggests that some heritable component of bipolar disorder overlaps with heritable components of creativity. Probands of people with bipolar disorder are more likely to be professionally successful, as well as to demonstrate temperamental traits similar to bipolar disorder. Furthermore, while studies of the frequency of bipolar disorder in creative population samples have been conflicting, studies that have a positive finding report that full blown bipolar disorder is rare.[184]
Specific populations
Children

Lithium is the only medication approved by the FDA for treating mania in children
In the 1920s, Emil Kraepelin noted that manic episodes are rare before puberty.[185] In general, bipolar disorder in children was not recognized in the first half of the twentieth century. This issue diminished with an increased following of the DSM criteria in the last part of the twentieth century.[185][186] The DSM5 does not specifically have bipolar disorder in children and instead refers to it as disruptive mood dysregulation disorder.[187]
While in adults the course of bipolar disorder is characterized by discrete episodes of depression and mania with no clear symptomatology between them, in children and adolescents very fast mood changes or even chronic symptoms are the norm.[188] Pediatric bipolar disorder is commonly characterized by outbursts of anger, irritability and psychosis, rather than euphoric mania, which is more likely to be seen in adults.[185][188] Early onset bipolar disorder is more likely to manifest as depression rather than mania or hypomania.[189]
The diagnosis of childhood bipolar disorder is controversial,[188] although it is not under discussion that the typical symptoms of bipolar disorder have negative consequences for minors suffering them.[185] The debate is mainly centered on whether what is called bipolar disorder in children refers to the same disorder as when diagnosing adults,[185] and the related question of whether the criteria for diagnosis for adults are useful and accurate when applied to children.[188] Regarding diagnosis of children, some experts recommend following the DSM criteria.[188] Others believe that these criteria do not correctly separate children with bipolar disorder from other problems such as ADHD, and emphasize fast mood cycles.[188] Still others argue that what accurately differentiates children with bipolar disorder is irritability.[188] The practice parameters of the AACAP encourage the first strategy.[185][188] American children and adolescents diagnosed with bipolar disorder in community hospitals increased 4-fold reaching rates of up to 40 percent in 10 years around the beginning of the 21st century, while in outpatient clinics it doubled reaching 6 percent.[188] Studies using DSM criteria show that up to 1 percent of youth may have bipolar disorder.[185]
Treatment involves medication and psychotherapy.[188] Drug prescription usually consists in mood stabilizers and atypical antipsychotics.[188] Among the former, lithium is the only compound approved by the FDA for children.[185] Psychological treatment combines normally education on the disease, group therapy and cognitive behavioral therapy.[188] Chronic medication is often needed.[188]
Current research directions for bipolar disorder in children include optimizing treatments, increasing the knowledge of the genetic and neurobiological basis of the pediatric disorder and improving diagnostic criteria.[188] Some treatment research suggests that psychosocial interventions that involve the family, psychoeducation, and skills building (through therapies such as CBT, DBT, and IPSRT) can benefit in a pharmocotherapy.[190] Unfortunately, the literature and research on the effects of psychosocial therapy on BPSD is scarce, making it difficult to determine the efficacy of various therapies.[190] The DSM-5 has proposed a new diagnosis which is considered to cover some presentations currently thought of as childhood-onset bipolar.[191]
Elderly
There is a relative lack of knowledge about bipolar disorder in late life. There is evidence that it becomes less prevalent with age but nevertheless accounts for a similar percentage of psychiatric admissions; that older bipolar patients had first experienced symptoms at a later age; that later onset of mania is associated with more neurologic impairment; that substance abuse is considerably less common in older groups; and that there is probably a greater degree of variation in presentation and course, for instance individuals may develop new-onset mania associated with vascular changes, or become manic only after recurrent depressive episodes, or may have been diagnosed with bipolar disorder at an early age and still meet criteria. There is also some weak and not conclusive evidence that mania is less intense and there is a higher prevalence of mixed episodes, although there may be a reduced response to treatment. Overall, there are likely more similarities than differences from younger adults.[192][193] In the elderly, recognition and treatment of bipolar disorder may be complicated by the presence of dementia or the side effects of medications being taken for other conditions.[194]
See also
Outline of bipolar disorder
Cyclothymia
Tristimania: A Diary of Manic Depression